The aorta is the largest artery in the human body. It carries oxygen-rich blood from the heart to the abdomen, pelvis, and legs.
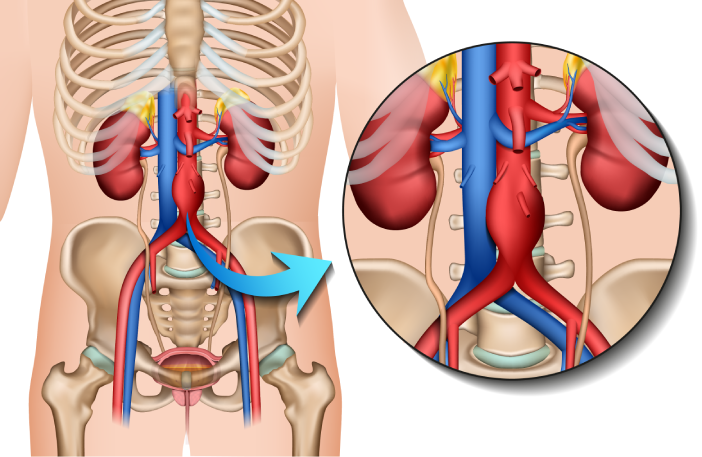
The abdominal portion of the aorta supplies vital organs and lower limbs. When the wall of this artery weakens, it can gradually dilate, forming an abdominal aortic aneurysm (AAA).
This dilation increases wall stress and, if left untreated, may lead to rupture — a life-threatening emergency. Because AAA often develops silently, understanding its circulatory role is essential for early detection.
An abdominal aortic aneurysm is a permanent and localized enlargement of the abdominal aorta, defined as a diameter 50% greater than normal.
AAA usually progresses slowly and may remain asymptomatic for years. The primary concern is the risk of rupture, which increases as the aneurysm enlarges.
Clinical classification showing progressive vessel dilation and increasing rupture risk
Several factors increase the likelihood of developing an abdominal aortic aneurysm:
Risk increases after 65
More common in men
Strongest modifiable risk factor
Weakens arterial walls
Plaque buildup in arteries
Genetic predisposition
Most AAAs are asymptomatic. When present, symptoms may include:
Immediate medical attention is required if sudden abdominal or back pain occurs, especially in patients with known aneurysms.
Early diagnosis allows safe monitoring and timely intervention.
Physical assessment may detect large aneurysms in some patients.
A non-invasive, painless examination used for screening, diagnosis, and follow-up.
Provides precise anatomical details for surgical planning or suspected complications.
Depend on aneurysm size, growth rate and patient condition.
Yes. The risk increases with aneurysm size and growth rate.
Risk can be reduced through smoking cessation and cardiovascular health management.
No. Abdominal ultrasound is painless and non-invasive.
Follow-up intervals depend on aneurysm size and growth.
Most patients have no symptoms until advanced stages.
Select your preferred clinic location and fill out the form. Our team will contact you shortly to confirm your appointment time.
Response within one business day (Closed Fridays)
Your data is secure
We welcome you to our two modern facilities in the Greater Montreal area.
239 Green Street
Saint-Lambert QC J4P1S9
450 259-1399
Free street parking available directly in front of the clinic
1065 Pratt Avenue
Outremont QC H2V 2V5
514 731-7757
Free street parking available directly in front of the clinic



